Airborne-mediated
microbial diseases such as influenza and tuberculosis represent major
public health challenges. A direct approach to prevent airborne
transmission is inactivation of airborne pathogens, and the airborne
antimicrobial potential of UVC ultraviolet light has long been
established; however, its widespread use in public settings is limited
because conventional UVC light sources are both carcinogenic and
cataractogenic. By contrast, we have previously shown that far-UVC light
(207–222 nm) efficiently inactivates bacteria without harm to exposed
mammalian skin. This is because, due to its strong absorbance in
biological materials, far-UVC light cannot penetrate even the outer (non
living) layers of human skin or eye; however, because bacteria and
viruses are of micrometer or smaller dimensions, far-UVC can penetrate
and inactivate them. We show for the first time that far-UVC efficiently
inactivates airborne aerosolized viruses, with a very low dose of
2 mJ/cm2 of 222-nm light inactivating >95% of aerosolized
H1N1 influenza virus. Continuous very low dose-rate far-UVC light in
indoor public locations is a promising, safe and inexpensive tool to
reduce the spread of airborne-mediated microbial diseases.
Introduction
Airborne-mediated microbial diseases represent one of the major challenges to worldwide public health1. Common examples are influenza2, appearing in seasonal3 and pandemic4 forms, and bacterially-based airborne-mediated diseases such as tuberculosis5, increasingly emerging in multi-drug resistant form.
A
direct approach to prevent the transmission of airborne-mediated
disease is inactivation of the corresponding airborne pathogens, and in
fact the airborne antimicrobial efficacy of ultraviolet (UV) light has
long been established6,7,8. Germicidal UV light can also efficiently inactivate both drug-sensitive and multi-drug-resistant bacteria9, as well as differing strains of viruses10.
However, the widespread use of germicidal ultraviolet light in public
settings has been very limited because conventional UVC light sources
are a human health hazard, being both carcinogenic and cataractogenic11,12.
By
contrast, we have earlier shown that far-UVC light generated by
filtered excimer lamps emitting in the 207 to 222 nm wavelength range,
efficiently inactivates drug-resistant bacteria, without apparent harm
to exposed mammalian skin13,14,15.
The biophysical reason is that, due to its strong absorbance in
biological materials, far-UVC light does not have sufficient range to
penetrate through even the outer layer (stratum corneum) on the surface
of human skin, nor the outer tear layer on the outer surface of the eye,
neither of which contain living cells; however, because bacteria and
viruses are typically of micron or smaller dimensions, far-UVC light can
still efficiently traverse and inactivate them13,14,15.
The earlier studies on the germicidal efficacy of far UVC light13,15,16,17,18
were performed exposing bacteria irradiated on a surface or in
suspension. In that a major pathway for the spread of influenza A is
aerosol transmission3,
we investigate for the first time the efficacy of far-UVC 222-nm light
for inactivating airborne viruses carried by aerosols – with the goal of
providing a potentially safe alternative to conventional 254-nm
germicidal lamps to inactivate airborne microbes.
Results
Virus inactivation
Figure 1
shows representative fluorescent 40× images of mammalian epithelial
cells incubated with airborne viruses that had been exposed in
aerosolized form to far-UVC doses (0, 0.8, 1.3 or 2.0 mJ/cm2)
generated by filtered 222-nm excimer lamps. Blue fluorescence was used
to identify the total number of cells in a particular field of view,
while green fluorescence indicated the integration of live influenza A
(H1N1) viruses into the cells. Results from the zero-dose control
studies (Fig. 1,
top left) confirmed that the aerosol irradiation chamber efficiently
transmitted the aerosolized viruses through the system, after which the
live virus efficiently infected the test mammalian epithelial cells.
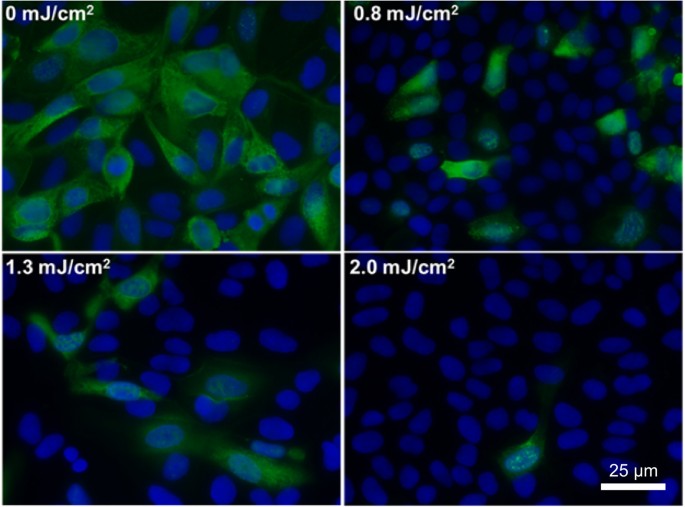
Figure 1
Antiviral
efficacy of different low doses of 222-nm far-UVC light. Typical
fluorescent images of MDCK epithelial cells infected with influenza A
virus (H1N1). The viruses were exposed in aerosolized form in the
irradiation chamber to doses of 0, 0.8, 1.3 or 2.0 mJ/cm2 of
222-nm far-UVC light. Infected cells fluoresce green (blue = nuclear
stain DAPI; green = Alexa Fluor-488 conjugated to anti-influenza A
antibody). Images were acquired with a 40× objective.
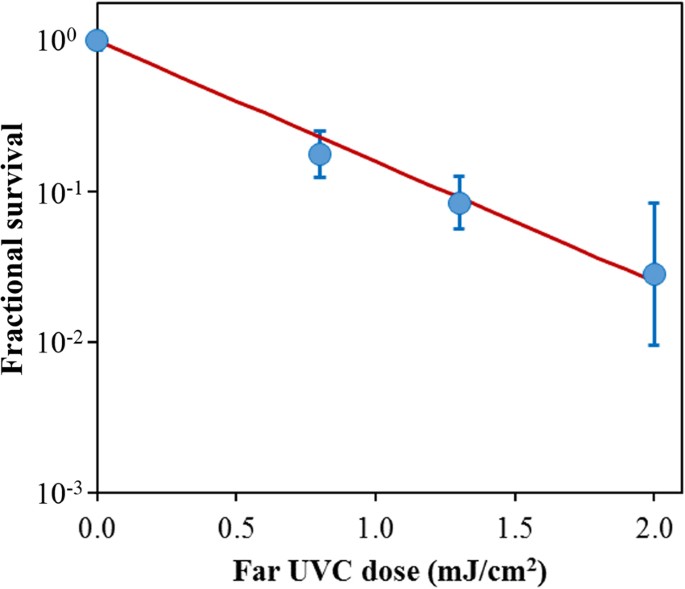
Figure 2
shows the surviving fraction, as a function of the incident 222-nm
far-UVC dose, of exposed H1N1 aerosolized viruses, as measured by the
number of focus forming units in incubated epithelial cells relative to
unexposed controls. Linear regressions (see below) showed that the
survival results were consistent with a classical exponential UV
disinfection model with rate constant k = 1.8 cm2/mJ (95% confidence intervals 1.5–2.1 cm2/mJ). The overall model fit was good, with a coefficient of determination, R2 = 0.95,
which suggests that most of the variability in virus survival was
explained by the exponential model. The rate constant of 1.8 cm2/mJ corresponds to an inactivation cross-section (dose required to inactivate 95% of the exposed viruses) of D95 = 1.6 mJ/cm2 (95% confidence intervals 1.4–1.9 mJ/cm2).
Figure 2
Quantification of the antiviral efficacy of 222-nm far-UVC light. Fractional survival, FFUUV/FFUcontrols,
is plotted as a function of the 222-nm far-UVC dose. Means and standard
deviations refer to triplicate repeat studies and the line represents
the best-fit regression to Eqn 1 (see text).
We
have developed an approach to UV-based sterilization using
single-wavelength far-UVC light generated by filtered excilamps, which
selectively inactivate microorganisms, but does not produce biological
damage to exposed mammalian cells and tissues13,14,15.
The approach is based on biophysical principles in that far-UVC light
can traverse and therefore inactivate bacteria and viruses which are
typically micrometer dimensions or smaller, whereas due to its strong
absorbance in biological materials, far-UVC light cannot penetrate even
the outer dead-cell layers of human skin, nor the outer tear layer on
the surface of the eye.
Here we applied this approach to test the
efficacy of the 222-nm far-UVC light to inactivate influenza A virus
(H1N1) carried by aerosols in a benchtop aerosol UV irradiation chamber,
which generated aerosol droplets of sizes similar to those generated by
human coughing and breathing. Aerosolized viruses flowing through the
irradiation chamber were exposed to UVC emitting lamps placed in front
of the chamber window.
As shown in Fig. 2,
inactivation of influenza A virus (H1N1) by 222-nm far-UVC light
follows a typical exponential disinfection model, with an inactivation
cross-section of D95 = 1.6 mJ/cm2 (95% CI:
1.4–1.9). For comparison, using a similar experimental arrangement, but
using a conventional 254 nm germicidal UVC lamp, McDevitt et al.19 found a D95 value of 1.1 mJ/cm2 (95% CI: 1.0–1.2) for H1N1 virus. Thus as we13,15 and others16,17,18
reported in earlier studies for bacterial inactivation, 222-nm far-UVC
light and 254-nm broad-spectrum germicidal light are also comparable in
their efficiencies for aerosolized viral inactivation. Other recent work
comparing viral inactivation across the UVC spectrum has shown
variations in efficiency are expected, but in general both regions of
the spectrum are effective in inactivation, though the precise cause of
inactivation may differ20,21.
However as discussed above, based on biophysical considerations and in
contrast to the known human health safety issues associated with
conventional germicidal 254-nm broad-spectrum UVC light, far-UVC light
does not appear to be cytotoxic to exposed human cells and tissues in vitro or in vivo13,14,15.
If
these results are confirmed in other scenarios, it follows that the use
of overhead low-level far-UVC light in public locations may represent a
safe and efficient methodology for limiting the transmission and spread
of airborne-mediated microbial diseases such as influenza and
tuberculosis. In fact the potential use of ultraviolet light for
airborne disinfection is by no means new, and was first demonstrated
more than 80 years ago8,22.
As applied more recently, airborne ultraviolet germicidal irradiation
(UVGI) utilizes conventional germicidal UVC light in the upper part of
the room, with louvers to prevent direct exposure of potentially
occupied room areas23.
This results in blocking more than 95% of the UV radiation exiting the
UVGI fixture, with substantial decrease in effectiveness24.
By contrast, use of low-level far-UVC fixtures, which are potentially
safe for human exposure, could provide the desired antimicrobial
benefits without the accompanying human health concerns of conventional
germicidal lamp UVGI.
A key advantage of the UVC based approach,
which is in clear contrast to vaccination approaches, is that UVC light
is likely to be effective against all airborne microbes. For example,
while there will almost certainly be variations in UVC inactivation
efficiency as different influenza strains appear, they are unlikely to
be large7,10.
Likewise, as multi-drug-resistant variants of bacteria emerge, their
UVC inactivation efficiencies are also unlikely to change greatly9.
In
conclusion, we have shown for the first time that very low doses of
far-UVC light efficiently inactivate airborne viruses carried by
aerosols. For example, a very low dose of 2 mJ/cm2 of 222-nm
light inactivates >95% of airborne H1N1 virus. Our results indicate
that far-UVC light is a powerful and inexpensive approach for prevention
and reduction of airborne viral infections without the human health
hazards inherent with conventional germicidal UVC lamps. If these
results are confirmed in other scenarios, it follows that the use of
overhead very low level far-UVC light in public locations may represent a
safe and efficient methodology for limiting the transmission and spread
of airborne-mediated microbial diseases. Public locations such as
hospitals, doctors’ offices, schools, airports and airplanes might be
considered here. This approach may help limit seasonal influenza
epidemics, transmission of tuberculosis, as well as major pandemics.
Methods
Far-UVC lamps
We used a bank of three excimer lamps containing a Kr-Cl gas mixture that predominantly emits at 222 nm25,26.
The exit window of each lamp was covered with a custom bandpass filter
designed to remove all but the dominant emission wavelength as
previously described15.
Each bandpass filter (Omega Optical, Brattleboro, VT) had a center
wavelength of 222 nm and a full width at half maximum (FWHM) of 25 nm
and enables >20% transmission at 222 nm. A UV spectrometer
(SPM-002-BT64, Photon Control, BC, Canada) with a sensitivity range
between 190 nm and 400 nm was utilized to verify the 222 nm emission
spectrum. A deuterium lamp standard with a NIST-traceable spectral
irradiance (Newport Model 63945, Irvine, CA) was used to radiometrically
calibrate the UV spectrometer. An SM-70 Ozone Monitor (Aeroqual,
Avondale, Auckland, New Zealand) measured the ozone generation from the
lamps to be <0.005 ppm, which is not a significant level to provide
an antimicrobial effect to aerosolized viruses27.
Far-UVC dosimetry
Optical
power measurements were performed using an 818-UV/DB low-power UV
enhanced silicon photodetector with an 843-R optical power meter
(Newport, Irvine, CA). Additional dosimetry to determine the uniformity
of the UV exposure was performed using far-UVC sensitive film as
described in our previous work28,29.
This film has a high spatial resolution with the ability to resolve
features to at least 25 µm, and exhibits a nearly ideal cosine response30,31. Measurements were taken between experiments therefore allowing placement of sensors inside the chamber.
A range of far-UVC exposures, from 3.6 µJ/cm2 up to 281.6 mJ/cm2,
were used to define a response calibration curve. Films were scanned as
48 bit RGB TIFF images at 150 dpi using an Epson Perfection V700 Photo
flatbed scanner (Epson, Japan) and analyzed with radiochromic film
analysis software32 to calculate the total exposure based on measured changes in optical density.
Measurements
using both a silicon detector and UV sensitive films were combined to
compute the total dose received by a particle traversing the exposure
window. The three vertically stacked lamps produced a nearly uniform
dose distribution along the vertical axis thus every particle passing
horizontally through the irradiation chamber received an identical dose.
The lamp width (100 mm) was smaller than the width of the irradiation
chamber window (260 mm) so the lamp power was higher near the center of
the irradiation chamber window compared to the edge. The UV sensitive
film indicated a power of approximately 120 µW/cm2 in the center third of the window and 70 µW/cm2
for the outer thirds. The silicon detector was used to quantify the
reflectivity of the aluminum sheet at approximately 15% of the incident
power. Combining this data allowed the calculation of the average total
dose of 2.0 mJ/cm2 to a particle traversing the window in
20 seconds. Additionally, the silicon detector was used to confirm the
attenuation of 222-nm light through a single sheet of plastic film was
65%. The addition of one or two sheets of plastic film between the lamps
and the irradiation chamber window yielded average doses of 1.3 mJ/cm2 and 0.8 mJ/cm2, respectively.
Benchtop aerosol irradiation chamber
A one-pass, dynamic aerosol / virus irradiation chamber was constructed in a similar configuration to that used by Ko et al.33, Lai et al.34, and McDevitt et al.19,35. A schematic overview of the system is shown in Fig. 3 and is pictured in Fig. 4.
Aerosolized viruses were generated by adding a virus solution into a
high-output extended aerosol respiratory therapy (HEART) nebulizer
(Westmed, Tucson, AZ) and operated using a dual-head pump (Thermo Fisher
420–2901–00FK, Waltham, MA) with an input flow rate of 11 L/min. The
aerosolized virus flowed into the irradiation chamber where it was mixed
with independently controlled inputs of humidified and dried air.
Humidified air was produced by bubbling air through water, while dry air
was provided by passing air through a desiccant air dryer (X06–02–00,
Wilkerson Corp, Richland, MI). Adjusting the ratio of humid and dry air
enabled control of the relative humidity (RH) within the irradiation
chamber which, along with the nebulizer settings, determined the aerosol
particle size distribution. An optimal RH value of 55% resulted in a
distribution of aerosol particle sizes similar to the natural
distribution from human coughing and breathing, which has been shown to
be distributed around approximately 1 µm, with a significant tail of
particles less than 1 µm36,37,38.